Interim Guidelines for COVID-19 Antibody Testing
Summary
Interim Guidelines for COVID-19 Antibody Testing
Serologic assays for SARS-CoV-2 now have Emergency Use Authorization (EUA) by the U.S. Food and Drug Administration (FDA), which has independently reviewed their performance.Serologic methods have been developed and will have important public health and clinical uses to monitor and respond to the COVID-19 pandemic.
- Currently, there is no identified advantage of assays whether they test for IgG, IgM and IgG, or total antibody.
- It is important to minimize false positive test results by choosing an assay with high specificity and by testing populations and individuals with an elevated likelihood of previous exposure to SARS-CoV-2. Alternatively, an orthogonal testing algorithm (i.e., employing two independent tests in sequence when the first test yields a positive result) can be used when the expected positive predictive value of a single test is low.
- Antibodies most commonly become detectable 1-3 weeks after symptom onset, at which time evidence suggests that infectiousness likely is greatly decreased and that some degree of immunity from future infection has developed. However, additional data are needed before modifying public health recommendations based on serologic test results, including decisions on discontinuing physical distancing and using personal protective equipment.
Background
Serologic assays for SARS-CoV-2, now broadly available, can play an important role in understanding the virus’s epidemiology in the general population and identifying groups at higher risk for infection. Unlike viral direct detection methods such as nucleic acid amplification or antigen detection tests that can detect acutely infected persons, antibody tests help determine whether the individual being tested was ever infected—even if that person never showed symptoms. Serologic tests detect waning or past SARS-CoV-2 virus infection indirectly, by measuring the host humoral immune response to the virus. Therefore, serology assays do not typically replace direct detection methods as the primary tool for diagnosing an active SARS-CoV-2 infection, but they do have several important applications in monitoring and responding to the COVID-19 pandemic.
Although serologic tests should not be used at this time to determine if an individual is immune, these tests can help determine the proportion of a population previously infected with SARS-CoV-2 and provide information about populations that may be immune and potentially protected. Thus, demographic and geographic patterns of serologic test results can help determine which communities may have experienced a higher infection rate and therefore may have higher rates of herd immunity. In some instances, serologic test results may assist with identifying persons potentially infected with SARS-CoV-2 and determining who may qualify to donate blood that can be used to manufacture convalescent plasmaexternal icon as a possible treatment for those who are seriously ill from COVID-19.
Development of Antibodies and Immunity
Nearly all immune competent individuals will develop an immune response following SARS-CoV-2 infection. Like infections with other pathogens, SARS-CoV-2 infection elicits development of IgM and IgG antibodies, which are the most useful for assessing antibody response because little is known about IgA response in the blood.
Antibodies in some persons can be detected within the first week of illness onset. SARS-CoV-2 infections are somewhat unusual because IgM and IgG antibodies arise nearly simultaneously in serum within 2 to 3 weeks after illness onset. Thus, detection of IgM without IgG is uncommon. How long IgM and IgG antibodies remain detectable following infection is not known.
In addition, development of neutralizing antibodies can also be assessed. Neutralizing antibodies inhibit viral replication in vitro, and as with many infectious diseases, their presence correlates with immunity to future infection, at least temporarily.
Recurrence of COVID-19 illness appears to be very uncommon, suggesting that the presence of antibodies could confer at least short-term immunity to infection with SARS-CoV-2. Consistent with this observation, experimental primary infection in primates and subsequent development of antibodies resulted in protection from reinfection after the primates were rechallenged. Additionally, antibody development in humans correlates with a marked decrease in viral load in the respiratory tract. Taken together, these observations suggest that the presence of antibodies may decrease a person’s infectiousness and offer some level of protection from reinfection. However, definitive data are lacking, and it remains uncertain whether individuals with antibodies (neutralizing or total) are protected against reinfection with SARS-CoV-2, and if so, what concentration of antibodies is needed to confer protection.
Current Status of Antibody Testing in the United States
Antigenic targets
The two major antigenic targets of SARS-CoV-2 virus against which antibodies are detected are spike glycoprotein (S) and nucleocapsid phosphoprotein (N). While S protein is essential for virus entry and is present on the viral surface, N protein is the most abundantly expressed immunodominant protein that interacts with RNA. Multiple forms of S protein — full-length (S1+S2) or partial (S1 domain or receptor binding domain [RBD]) — are used as antigens. The protein target determines cross-reactivity and specificity because N is more conserved across coronaviruses than S, and within S, RBD is more conserved than S1 or full-length S.
Types of Antibody Testing
Different types of assays can be used to determine different aspects of immune response and functionality of antibodies. The tests can be broadly classified to detect either binding or neutralizing antibodies.
- Binding antibody detection: These tests use purified proteins of SARS-CoV-2, not live virus, and can be performed in lower biosafety level laboratories (e.g., BSL-2). With specific reagents, individual antibody types, like IgG, IgM, and IgA, can be determined. In general, IgM is one of the first types of antibodies produced after infection and is most useful for determining recent infection, while IgG generally develops after IgM and may remain detectable for months or years. IgA is important for mucosal immunity and can be detected in mucous secretions like saliva in addition to blood, though its significance in this disease is still to be determined. Depending on the complexity of assays, these tests can be performed rapidly (less than 30 minutes) in a field setting or in a few hours in a laboratory.
Tests that detect binding antibodies fall into two broad categories.
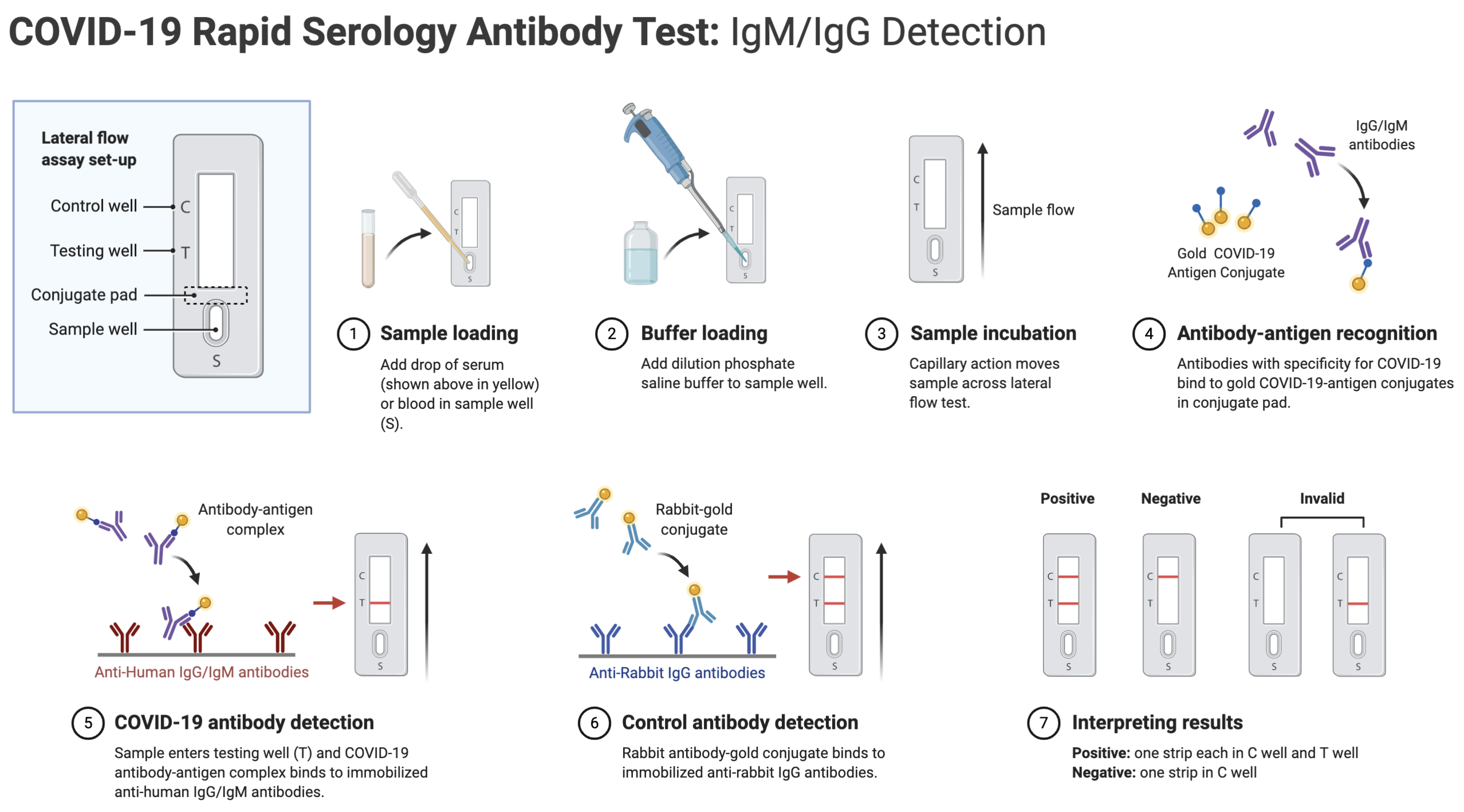
- Point-of-care (POC) tests generally are lateral flow devices that detect IgG or IgG and IgM, or total antibody in serum, plasma, whole blood, and/or saliva. An advantage of some point-of-care tests using whole blood is that they can be performed on blood samples obtained by fingerstick rather than venipuncture.
- Laboratory tests use ELISA (Enzyme-Linked Immunosorbent Assay) or CIA (chemiluminescent immunoassay) methods for antibody detection, which for some assays may require trained laboratorians and specialized instruments. Based on the reagents, IgG, IgM, and IgA can be detected separately or combined as total antibody.
- Neutralizing antibody detection: FDA has not yet authorized the use of neutralization tests for SARS-CoV-2. Neutralization tests determine the functional ability of antibodies to prevent infection of virus in vitro. The test involves incubating serum or plasma with live virus followed by infection and incubation of cells. Testing will require either BSL-3 or BSL-2 laboratories, depending on what form of the SARS-CoV-2 virus is used.
Two types of neutralization tests are conducted.
- Virus neutralization tests (VNT), such as the plaque-reduction neutralization test (PRNT) and microneutralization, use a SARS-CoV-2 virus from a clinical isolate or recombinant SARS-CoV-2 expressing reporter proteins. This testing requires BSL-3 laboratories and may take up to 5 days to complete.
- Pseudovirus neutralization tests (pVNT) use recombinant pseudoviruses (like vesicular stomatitis virus, VSV) that incorporate the S protein of SARS-CoV-2. This testing can be performed in BSL-2 laboratories depending on the VSV strain used.
FDA-authorized serologic tests
FDA now requires commercially marketed serologic tests to receive Emergency Use Authorization (EUA)external icon. Tests that are not commercially marketed do not require FDA authorization but developers may voluntarily request authorization. Multiple agencies — including FDA, the National Cancer Institute/National Institutes of Health (NCI/NIH), CDC, and the Biomedical Advanced Research and Development Authority (BARDA) — are collaborating with members of academia and the medical community to evaluate several serology tests using a well-characterized set of clinical samples (serum or plasma) collected before and during the current COVID-19 outbreak. A list of all tests authorized for emergency use under EUA is maintained on an FDA website external icon. All currently authorized tests are qualitative (providing a result that is positive, negative, or indeterminate) rather than quantitative (providing a quantitative assessment of antibody levels).
Both laboratory and rapid serologic assays have received EUA. Serologic testing technologies include single-use, low-throughput lateral flow tests where the presence of antibody is demonstrated by a color change on a paper strip and laboratory-based immunoassays that allow for processing of many samples at the same time.
The EUA letter of authorization includes the settings in which the test is authorized, based on FDA’s determination of appropriate settings for use during the public health emergency.
Optimizing Testing Outcomes
Test performance
The utility of tests depends on the sensitivity and specificity of the assays; these performance characteristics are determined by using a defined set of negative and positive samples. In addition, the predictive values of a test should be considered because these values affect the overall outcome of testing. Positive predictive value is the probability that individuals with positive test results are truly antibody positive. Negative predictive value is the probability that individuals with negative test results are truly antibody negative. Positive and negative predictive values are determined by the percentage of truly antibody positive individuals in the tested population (prevalence, pre-test probability) and the sensitivity and specificity of the test. For example:
- In a high-prevalence setting, the positive predictive value increases — meaning it is more likely that persons who test positive are truly antibody positive – than if the test is performed in a population with low-prevalence. When a test is used in a population where prevalence is low, the positive predictive value drops because there are more false-positive results, since the pre-test probability is low.
- Likewise, negative predictive value is also affected by prevalence. In a high-prevalence setting, the negative predictive value declines whereas in a low-prevalence setting, it increases.
In most of the country, including areas that have been heavily impacted, the prevalence of SARS-CoV-2 antibody is expected to be low, ranging from <5% to 25%, so that testing at this point might result in relatively more false positive results and fewer false-negative results.
In some settings, such as COVID-19 outbreaks in food processing plants and congregate living facilities, the prevalence of infection in the population may be significantly higher. In such settings, serologic testing at appropriate intervals following outbreaks might result in relatively fewer false positive results and more false-negative results.
Testing strategies
In the current pandemic, maximizing specificity and thus positive predictive value in a serologic algorithm is preferred in most instances, since the overall prevalence of antibodies in most populations is likely low. For example, in a population where the prevalence is 5%, a test with 90% sensitivity and 95% specificity will yield a positive predictive value of 49%. In other words, less than half of those testing positive will truly have antibodies. Alternatively, the same test in a population with an antibody prevalence exceeding 52% will yield a positive predictive greater than 95%, meaning that less than one in 20 people testing positive will have a false positive test result.
Three strategies can be used to improve positive predictive value:
- Choosing a test with a very high specificity, perhaps 99.5% or greater, will yield a high positive predictive value in populations tested with prevalence >5%.
- Another strategy is to focus testing on persons with a high pre-test probability of having SARS-CoV-2 antibodies, such as persons with a history of COVID-19-like illness.
- A third approach is to employ an orthogonal testing algorithm in which persons who initially test positive are tested with a second test. Effective orthogonal algorithms are generally based on testing a patient sample with two tests, each with unique design characteristics (e.g., antigens or formats).
Algorithms can be designed to maximize overall specificity while retaining maximum sensitivity. For example, in the example above with a population prevalence of 5%, a positive predictive value of 95% can be achieved if samples initially positive are tested with a second different orthogonal assay that also has 90% sensitivity and 95% specificity. The performance of orthogonal testing algorithms has not been systematically evaluated but can be estimated using an on-line calculator external icon from the FDA. See Table 1 for the potential improvement benefits of the orthogonal testing algorithm.
Limitations of Serologic Tests
At present, the immunologic correlates of immunity from SARS-CoV-2 infection are not well defined. Representatives from BARDA, CDC, FDA, NIH, the Office of the Assistant Secretary for Health (OASH), Department of Defense (DoD), and White House Office of Science and Technology Policy (OSTP) are working with members of academia and the medical community to determine whether positive serologic tests are indicative of protective immunity against SARS-CoV-2. This work includes assessing the level of antibodies required for protection from reinfection, the duration of that protection, and the factors associated with development of a protective antibody response. The kinetics of antibody response, longevity of antibodies, the ability of antibodies to protect from repeat infection, the protective titer of neutralizing antibody, and the correlation of binding antibody titers to neutralization ability are yet to be determined. Although animal challenge studies demonstrate protection in the short run, demonstration of long-term protection in humans will require future study. Hence, pending additional data, the presence of antibodies cannot be equated with an individual’s immunity from SARS-CoV-2 infection.
Some tests may exhibit cross-reactivity with other coronaviruses, such as those that cause the common cold. This could result in false-positive test results. Some persons may not develop detectable antibodies after coronavirus infection. In others, it is possible that antibody levels could wane over time to undetectable levels. IgM and IgG antibodies are not present early in infection. Thus, serologic test results do not indicate with certainty the presence or absence of current or previous infection with SARS-CoV-2.